Rohingya Refugee Camps in the Cox's Bazaar District of Bangladesh are experiencing an acute surge in dengue cases as compared to the previous four years (2018 to 2021), according to a press release issued by the World Health Organization on 3 August 2022. As of 24 July, a total of 7687 confirmed cases and 6 deaths have been reported in 2022, with 93% (7178) of the cumulative number of cases being reported since the start of the surge at the end of May. Dengue is endemic in Bangladesh, but a similar surge has not been observed in the larger Cox’s Bazar district outside of the Rohingya Refugee Camps nor at the national level with case numbers and trends within expected levels of incidence for the same period. As dengue is recurrent in this part of the country, the population may be at risk of secondary infection, which puts them at higher risk for severe disease.
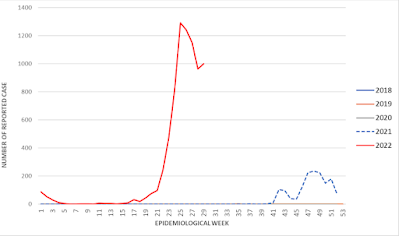
Rapid diagnostic test-confirmed cases of Dengue Fever in Rohingya Refugee Camps in Cox’s Bazar District, Bangladesh by notification date, 1 January 2018 to 24 July 2022. World Health Organization.
From 1 January to 24 July 2022, a total of 7687 cases of Dengue, confirmed by rapid diagnostic test (RDT), and six deaths (case fatality rate, 0.08%) have been reported from the Rohingya Refugee Camps in the Ukhia Upazila and Teknaf Upazila (sub-districts) of Cox’s Bazar, with the former sub-district being the most affected of the two. An acute surge of cases began during the week commencing 23 May, and peaked the week ending 26 June, with 93% (7178) of the cumulative number of cases being reported between 23 May and 24 July. A decreasing trend in reported Dengue cases was observed following the peak.
Cases of reported Dengue in Rohingya Refugee Camps are significantly higher as compared to similar periods over the past four years; 2018 (4 cases), 2019 (7 cases), 2020 (3 cases), and 2021 (1530 cases and 3 deaths with a surge from October to December). However, at a national level and in the larger Cox’s Bazar district, case numbers have been within expected endemic levels of incidence; by comparison to the Dengue case from the camps, the larger Cox’s Bazar district reported approximately 121 cases from 1 January to the end of June.
Camps located in Ukhia Upazila are predominantly affected by the outbreak. Camp 3 accounted for over 50% of all reported cases and Camps 4 and 1W each account for less than 10% of cases as of 24 July 2022. More than two-thirds of cases (67%) were among persons 15 years and older with males accounting for 60% of cases. The majority of cases (81%) were hemodynamically stable, i.e. not showing any warning signs for Severe Dengue Syndrome (such as Dengue Hemorrhagic Fever or Dengue Shock Syndrome) nor having any coexisting conditions, while approximately 15% of cases were mild and required observation and admission to primary health facilities. Severe Dengue with signs of Dengue Hemorrhagic Fever and Dengue Shock Syndrome was observed in 0.3% of cases and required admission to Cox’s Bazar District Hospital located within the camp. Among patients admitted to the hospital, 1% required blood transfusion. Previous Dengue infection was reported in 1% of current cases.
Serotyping results from 10 samples processed at the Institute of Epidemiology, Disease Control and Research reference laboratory in the capital Dhaka identified Dengue Fever Virus-3 (5 samples) and Dengue Fever Virus-2 (3 samples). Two samples had inconclusive results.
Dengue is endemic in Bangladesh with recurrent outbreaks. The Rohingya Refugee Camps in Cox’s Bazar district previously experienced an acute Dengue outbreak from October to December 2021 during which 1530 cases, including 3 deaths, were reported. Case numbers began to decline at the beginning of 2022, and by the end of February, the event was under control until the resurgence of cases in May 2022.
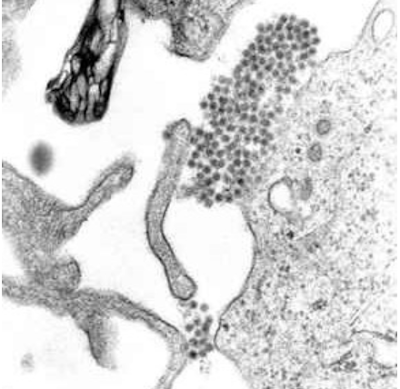
Dengue is a viral infection transmitted to humans through the bite of infected Mosquitoes and is found in tropical and sub-tropical climates worldwide, mostly in urban and semi-urban areas. The primary vectors that transmit the disease are Aedes aegypti mosquitoes and, to a lesser extent, Aedes albopictus. These mosquitoes are also vectors of Chikungunya, Yellow Fever and Zika viruses. Dengue is widespread throughout the tropics, with local variations in risk influenced by climate parameters as well as social and environmental factors.
Dengue causes a wide spectrum of disease. This can range from subclinical disease (people may not know they are even infected) to severe flu-like symptoms in those infected. Although less common, some people develop Severe Dengue, which can be any number of complications associated with severe bleeding, organ impairment and/or plasma leakage. Severe Dengue has a higher risk of death when not managed appropriately. Severe Dengue was first recognised in the 1950s during Dengue epidemics in the Philippines and Thailand. Today, Severe Dengue affects most Asian and Latin American countries and has become a leading cause of hospitalisation and death among children and adults in these regions.
Dengue is caused by a Virus of the Flaviviridae family and there are four distinct, but closely related, serotypes of the Virus that cause Dengue (Dengue Fever Virus-1, Dengue Fever Virus-2, Dengue Fever Virus-3 and Dengue Fever Virus-4). Recovery from infection is believed to provide lifelong immunity against that serotype. However, cross-immunity to the other serotypes after recovery is only partial, and temporary. Subsequent infections (secondary infection) by other serotypes increase the risk of developing Severe Dengue.
Dengue has distinct epidemiological patterns, associated with the four serotypes of the Virus. These can co-circulate within a region, and indeed many countries are hyper-endemic for all four serotypes. Dengue has an alarming impact on both human health and the global and national economies. Dengue Fever Virus is frequently transported from one place to another by infected travellers; when susceptible vectors are present in these new areas, there is the potential for local transmission to be established.
The incidence of Dengue has grown dramatically around the world in recent decades. A vast majority of cases are asymptomatic or mild and self-managed, and hence the actual numbers of dengue cases are under-reported. Many cases are also misdiagnosed as other febrile illnesses
One modelling estimate indicates 390 million Dengue Virus infections per year, of which 96 million manifest clinically (with any severity of disease). Another study on the prevalence of dengue estimates that 3.9 billion people are at risk of infection with dengue viruses. Despite a risk of infection existing in 129 countries, 70% of the actual burden is in Asia.
The number of dengue cases reported to the World Health Organization increased over 8 fold over the last two decades, from 505 430 cases in 2000, to over 2.4 million in 2010, and 5.2 million in 2019. Reported deaths between the year 2000 and 2015 increased from 960 to 4032, affecting mostly younger age group. The total number of cases seemingly decreased during years 2020 and 2021, as well as for reported deaths. However, the data is not yet complete and COVID-19 pandemic might have also hampered case reporting in several countries.
The overall alarming increase in case numbers over the last two decades is partly explained by a change in national practices to record and report Dengue to the Ministries of Health, and to the World Health Organization. But it also represents government recognition of the burden, and therefore the pertinence to report Dengue disease burden.
Before 1970, only 9 countries had experienced Severe Dengue epidemics. The disease is now endemic in more than 100 countries in the World Health Organization regions of Africa, the Americas, the Eastern Mediterranean, South-East Asia and the Western Pacific. The Americas, South-East Asia and Western Pacific regions are the most seriously affected, with Asia representing about 70% of the global burden of disease.
Not only is the number of cases increasing as the disease spreads to new areas including Europe, but explosive outbreaks are occurring. The threat of a possible outbreak of Dengue now exists in Europe; local transmission was reported for the first time in France and Croatia in 2010 and imported cases were detected in 3 other European countries. In 2012, an outbreak of Dengue on the Madeira islands of Portugal resulted in over 2000 cases and imported cases were detected in mainland Portugal and 10 other countries in Europe. Autochthonous cases are now observed on an annual basis in few European countries.
The largest number of dengue cases ever reported globally was in 2019. All regions were affected, and Dengue transmission was recorded in Afghanistan for the first time. The American region alone reported 3.1 million cases, with more than 25 000 classified as severe. Despite this alarming number of cases, deaths associated with Dengue were fewer than in the previous year. High number of cases were reported in Bangladesh (101 000), Malaysia (131 000) Philippines (420 000), Vietnam (320 000) in Asia.
In 2020, Dengue affected several countries, with reports of increases in the numbers of cases in Bangladesh, Brazil, Cook Islands, Ecuador, India, Indonesia, Maldives, Mauritania, Mayotte (France), Nepal, Singapore, Sri Lanka, Sudan, Thailand, Timor-Leste and Yemen. Dengue continues to affect Brazil, India, Vietnam, the Philippines, Cook Islands, Colombia, Fiji, Kenya, Paraguay, Peru and, Reunion islands, in 2021.
The COVID-19 pandemic is placing immense pressure on health care and management systems worldwide. The World Health Organization has emphasised the importance of sustaining efforts to prevent, detect and treat vector-borne diseases during this pandemic such as Dengue and other Arboviral diseases, as case numbers increase in several countries and place urban populations at highest risk for both diseases. The combined impact of the COVID-19 and dengue epidemics could have devastating consequences on the populations at risk.
The virus is transmitted to humans through the bites of infected female Mosquitoes, primarily the Aedes aegypti Mosquito. Other species within the Aedes genus can also act as vectors, but their contribution is secondary to Aedes aegypti.
After feeding on an Dengue Fever Virus-infected person, the virus replicates in the Mosquito midgut, before it disseminates to secondary tissues, including the salivary glands. The time it takes from ingesting the Virus to actual transmission to a new host is termed the extrinsic incubation period. The extrinsic incubation period takes about 8-12 days when the ambient temperature is between 25-28°C. Variations in the extrinsic incubation period are not only influenced by ambient temperature; a number of factors such as the magnitude of daily temperature fluctuations, Virus genotype, and initial viral concentration, can also alter the time it takes for a Mosquito to transmit Virus. Once infectious, the Mosquito is capable of transmitting Virus for the rest of its life.
Mosquitoes can become infected from people who are viremic with Dengue Fever Virus. This can be someone who has a symptomatic Dengue infection, someone who is yet to have a symptomatic infection (they are pre-symptomatic), but also people who show no signs of illness as well (they are asymptomatic).
Human-to-Mosquito transmission can occur up to 2 days before someone shows symptoms of the illness, up to 2 days after the fever has resolved. Risk of Mosquito infection is positively associated with high viremia and high fever in the patient; conversely, high levels of Dengue Fever Virus-specific antibodies are associated with a decreased risk of Mosquito infection. Most people are viremic for about 4-5 days, but viremia can last as long as 12 days.
The primary mode of transmission of Dengue Fever Virus between Humans involves Mosquito vectors. There is evidence however, of the possibility of maternal transmission (from a pregnant mother to her baby). While vertical transmission rates appear low, with the risk of vertical transmission seemingly linked to the timing of the Dengue infection during the pregnancy. When a mother does have a Dengue Fever Virus infection when she is pregnant, babies may suffer from pre-term birth, low birthweight, and fetal distress.
Rare cases of transmission via blood products, organ donation and transfusions have been recorded. Similarly, transovarial transmission (i.e. the transmission of the Virus from a female Mosquito to her young) of the Virus within Mosquitoes have also been recorded.
The Aedes aegypti mosquito is considered the primary vector of Dengue Fever Virus. It could breed in natural containers such as tree holes and Bromeliads, but nowadays it has well adapted to urban habitats and breeds mostly in man-made containers including buckets, mud pots, discarded containers and used tyres, storm water drains etc., thus making Dengue an insidious disease in densely populated urban centres. Aedes aegypti is a day-time feeder; its peak biting periods are early in the morning and in the evening before sunset. Female Aedes aegypti frequently feed multiple times between each egg-laying period leading to clusters of infected individuals. Once a female has laid her eggs, these eggs can remain viable for several months in dry condition, and will hatch when they are in contact with water.

Colour print of the Dengue Mosquito Aedes aegypti (then called Stegomyia fasciata, today also Stegomyia aegypti). To the left, the male, in the middle and on the right, the female. Above left, a flying pair in copula. Emil August Goeldi (1905)/Wikimedia Commons.
Aedes albopictus, a secondary Dengue vector and, has spread to more than 32 states in the USA, and more than 25 countries in the European Region, largely due to the international trade in used tyres (a breeding habitat) and other goods (e.g. lucky Bamboo). It favours breeding sites close to dense vegetation including plantations which is linked to increased risk of exposure for rural workers such as those in Rubber and Palm Oil plantation, but it is also found to be established abundantly in urban areas. Aedes albopictus is highly adaptive. Its geographical spread is largely due to its tolerance of colder conditions, as an egg and adult. Similar to Aedes aegypti, Aedes albopictus is also a day biter and it has been implicated as the primary vector of Dengue Fever Virus in a limited number of outbreak, where Aedes aegypti is either not present, or present in low numbers.
While majority of Dengue cases are asymptomatic or show mild symptoms, it can manifest as a severe, flu-like illness that affects infants, young children and adults, but seldom causes death. Symptoms usually last for 2–7 days, after an incubation period of 4–10 days after the bite from an infected Mosquito. The World Health Organization classifies Dengue into 2 major categories: Dengue (with or without warning signs) and Severe Dengue. The sub-classification of Dengue with or without warning signs is designed to help health practitioners triage patients for hospital admission, ensuring close observation, and to minimise the risk of developing Severe Dengue.
See also...
Follow Sciency Thoughts on Facebook.
Follow Sciency Thoughts on Twitter.










%20(1)%20(1).png)



















-by-date-of-symptom-onset-in-the-united-republic-of-tanzania--as-of-31-may-2023.png)