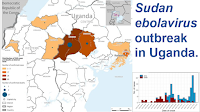
On 1 June 2020 medical authorities in Équateur Province, Democratic Republic of the Congo, reported an outbreak of Ebolavirus Disease in Mbandaka, the capital of Équateur Province. This was the eleventh reported outbreak of an Ebola-type disease in the Democratic Republic of the Congo, and was close to the location of a previous outbreak in the Bikoro health zone of Équateur Province, which occurred in 2018. The Democratic Republic of the Congo suffered fifteen outbreaks of Ebola-type diseases between 1 September 1976 and 22 August 2022, with the 2020 Équateur Province outbreak being the eleventh of these. The majority of these were caused by the Ebolavirus, and occurred in the north of the country, although one, in Haut-Uélé Province in 2012, was caused by the Bundibugyo Virus.
Ebolavirus has not been found in Bats in the Democratic Republic of the Congo, but the closely related Marburg Virus has, and Bats with antibodies to Ebolavirus have been found in Nord Kivu Province and Équateur provinces, as well as in the neighbouring Republic of Congo. Outbreaks of Ebola have been associated with the handling of Chimpanzees and Gorillas in the Republic of Congo and Gabon, and Ape populations have been known suffer dramatic declines at the same time as local Human populations have suffered outbreaks of Ebola-type diseases. Furthermore, as with other Filoviruses, Ebolavirus can persist in the system of survivors after they have apparently recovered, and cause new infections via sexual transmission or other exchange of bodily fluids. Before it became possible to identify Ebolaviruses by rapid genetic sequencing, it was impossible to tell whether outbreaks of the disease were caused by new infections from zoonotic sources (i.e. Animals) or transmission from apparently heathy survivors.
In a paper published in the journal The Lancet Microbe on 23 January 2024, a team of scientists led by Eddy Kinganda-Lusamaki of the Pathogen Genomics Laboratory at the Institut National de Recherche Biomédicale in Kinshasa, the Faculté de Médecine at the Université de Kinshasa, and the Institut de Recherche pour le Développement at the University of Montpellier, present the results of an assessment of the epidemiological and genetic properties of the 2020 Équateur Province Ebola outbreak.
The 2020 Équateur Province outbreak was the Democratic Republic of the Congo's eleventh Ebola outbreak, and started while the tenth outbreak, in North Kivu Province, was still ongoing. This led to suspicions that the two events were related, with the Équateur Province potentially being caused by an infected person travelling from North Kivu. Kinganda-Lusamaki et al. were able to demonstrate that this was not the case, with the two outbreaks being caused by different strains of Ebolavirus, and the Équateur Province outbreak having a zoonotic origin.

Ebolavirus outbreaks in the Democratic Republic of the Congo, 1976–2022. (A) The distribution of Ebolavirus disease outbreaks in the Democratic Republic of the Congo. Coloured circles identify locations of previous outbreaks and the size of circles represents the number of positive Human cases. The map shows the affected 2020 health zones (orange and purple shading) and sites of the 2018 Équateur outbreak (orange shading). The red star indicates the location of the Kinshasa diagnostic laboratory during the Équateur Province 2020 outbreak. (B) The locations and prevalence of Ebolavirus disease cases during the 2020 Ebola virus disease outbreak in the Équateur Province. The red stars indicate the location of the diagnostic and field laboratories during the Équateur Province 2020 outbreak (Mbandaka, Ingende, Itipo, Bikoro, and Bolomba). Kinganda-Lusamaki et al. (2024).
Blood samples from live patients with suspected Ebola and oral swabs from deceased patients thought to have died of Ebola were tested for signs of the Virus. Unlike in previous outbreaks, the presence of a fever was not required for patients to be included in the suspected group, since it has been demonstrated that not all people infected with Ebolavirus develop a fever.
Between 19 May and 16 September 2020, 130 probable cases of Ebola were reported in., 119 of which were confirmed by laboratory analysis. Of the 130 suspected cases, 55 died, a case fatality rate of 42%. Cases were reported in thirteen health zones, Bikoro, Bolenge, Bolomba, Bomongo, Iboko, Ingende, Lilanga Bobangi, Lolanga Mampoko, Lotumbe, Mkanza, Mbandaka, Monieka, and Wangata. The epidemic declined rapidly after August, with the last case being reported on 12 September. Thhe highest number of infections was among men in the 45 or older age bracket, while the least affected group were children aged 5-14. This is surprising, as Équateur Province has a young population, with many more children than older men. This was particularly true in the early stages of the epidemic, with no individuals of 15 or younger affected in May or June, while several children were infected between July and September. The date of the first onset of symptoms was identified for all cases. Forty seven infected persons visited more one health clinic after the onset of symptoms, with three individuals visiting four separate health clinics. The earliest identified case was a 37-year-old woman identified as a housewife, residing in the Mbandaka health zone, who had no contact with any known earlier case, but who was known to have consumed wild Bat meat, strongly suggesting a zoonitic origin for the epidemic.

Demographics of Ebolavirus Disease cases during the 2020 Équateur Province outbreak (A) Epidemiological curve of confirmed and probable Ebolavirus Disease cases over time. (B) Age distribution of confirmed and probable Ebolavirus Disease cases by gender (the black horizontal bars represent the 2020 Democratic Republic of the Congo known age and gender population distribution from the World Health Organization). (C) Temporal age distribution of individuals with Ebolavirus Disease. (D) Distribution of patients with Ebolavirus Disease who visited multiple health-care facilities after symptoms onset. Kinganda-Lusamaki et al. (2024). Three of the people infected during the epidemic were healthcare workers, and one a traditional healer. Two of these died. Thirty seven of the infected were described as farmers, fishers, or hunters, 25 as housewives, and seven as businesspeople. Ninety four of the infected people are known to have had contact with another known case before becoming infected. Nine reported having contact with an unidentified person who they thought might be infected, 23 had no known link to another case, and four reported contact with Animals which may have passed on the infection.
Nineteen of the infected are believed to have contracted the Virus from a member of their household, twenty from another member of their community, twelve people are thought to have contracted the Virus at a funeral. Twenty seven patients reported multiple potential contact sources, in 44 cases the route of exposure was unknown.
While it was not possible to obtain specimens from all patients, Kinganda-Lusamaki et al. were able to obtain 188 specimens from 122 of the patients, from which they were able to sequence 87 viral genomes. This led to the discovery that there were in fact two separate variants of the Virus circulating during the epidemic, with 83 of the genomes belonging to the Mbandaka variant of the Virus and three belonging to the Tumba variant; a partial sequence (defined as a sequence where less than 70% of the Viruses DNA was recovered) obtained from another patient was also identified as belonging to the Tumba variant. All of the Mbandaka variant cases were calculated to have descended from a last common ancestor which probably existed in a non-Human host in January 2020, with two separate instances of the Virus jumping to Human hosts and then spreading within the community. The first known example of the Tumba variant in the 2020 outbreak was a nineteen-year-old man who visited two separate healthcare clinics before being diagnosed. This patient had no-known contact with any earlier patient, nor had he consumed bushmeat or had contact with any wild or domestic Animals. All three subsequent cases had had contact with this initial case. The previous outbreak of Ebola in Équateur Province in 2018 was also the Tumba variant of the Virus, although it was impossible to determine whether the new outbreak was due to a persistent infection from the earlier epidemic.
By using patient-generated data, Kinganda-Lusamaki et al. were able to generate a history of the 2020 Ebolavirus outbreak in Équateur Province, Democratic Republic of the Congo, which included genetic data, records of health centre visits, dates of infection, identification of the Virus, isolation of patients, and deaths. This enabled them to plot chains of infection, with nineteen chains of infection being determined before generic data was incorporated into the study, and eighteen of these subsequently being stitched together with genetic data to form the Mbandaka variant tree. Twenty of the patients had no determined route of infection, with eleven of these also subsequently added to the Mbandaka variant tree from genetic data; genetic data was not available from the remaining nine patients. Three individuals reported that believing they had contracted the Virus from contact with Animals, but were demonstrated to be part of the Human-to-Human chain of Mbandaka variant infection. Two individuals were identified from samples taken when they visited healthcare clinics for reasons unrelated to Ebolavirus; both went on to develop symptoms of the disease.
Kinganda-Lusamaki et al. were able to develop an extensive overview of the 2020 Ebolavirus outbreak in Équateur Province, but caution that this data is still probably incomplete, with cases for which the infection routes were unknown or only probable, making it likely that there were other, unidentified cases within the community. A similar pattern was observed in the concurrent epidemic in North Kivu Province. The outbreak appeared to start with an individual who consumed Bat meat, and was of a newly identified strain of the Ebolavirus, identified as the Mbandaka variant. A minority of the cases belonged to a second strain, the Tumba variant, which caused an epidemic of the disease in 2018, and appeared to re-emerge from a survivor in 2020. The Équateur Province outbreak was found to be unrelated to the concurrent North Kivu Province epidemic, contrary to expectations. Their hope is that by utilising both social and genetic data to understand the transmission of the Virus their study will enable healthcare workers to be able to better manage future outbreaks of Ebolavirus.
Kinganda-Lusamaki et al. identified several different routes of Ebolavirus infection during the 2020 outbreak, including zoonotic transmission from Animals, person-to-person infection due to close contact with infected individuals, and the re-emergence of the Virus from a persistent infection. The ability of the Virus to re-emerge as a persistent infection from apparently healthy individuals after quite long intervals has proven to be a problem in other Ebolavirus outbreaks elsewhere in the Democratic Republic of the Congo, as well as in Guinea. This can be differentiated from fresh zoonotic infections by genetic testing (the persistent infection will be genetically close to the previous outbreak, whereas a fresh zoonotic infection is likely to have a novel genome, forming their own distinct clade of infections.
Research around the 2014 Ebolavirus outbreak in Guinea, Sierra Leone, and Liberia demonstrated the importance of educating survivors of the disease of the potential dangers of transmitting the disease after all symptoms have passed, something which Kinganda-Lusamaki et al.'s emphasise.
In the 2020 Équateur Province it took an average of six days between the onset of symptoms and patients being isolated within medical facilities (which was quite often longer than the patient lived), as a consequence, many patients visited multiple healthcare facilities, increasing the number of other people they came into contact with. Based upon this, Kinganda-Lusamaki et al. strongly recommend that in future outbreaks a system of rapid testing is introduced as quickly as possible. They note that an enhanced viral haemorrhagic fever surveillance programme has helped the country to respond rapidly to several outbreaks of different haemorrhagic diseases (including Marburg Virus Disease, Crimean-Congo haemorrhagic fever, and Rift Valley fever), resulting in the severity and duration of the outbreaks being reduced. A similar system would enable the Democratic Republic of the Congo to respond in the same way.
During the last three weeks of the 2020 Équateur Province outbreak, cases were limted to six healthcare districts, falling to two in the last two weeks. Eight of the thirteen new cases reported in the last three weeks were children under fourteen years of age, possibly suggesting that the majority of older people in the area by this time were producing antibodies to the disease, either as a result of prior exposure or vaccination. During the outbreak the rVSVΔG-ZEBOV-GP vaccine was administered to all known contacts of patients who were more than six months old, as part of a ring vaccination strategy. Unfortunately, record keeping was imperfect, and it is unclear if the reported cases in the last few weeks had been vaccinated, or whether they had been in contact with unvaccinated people. During the North Kivu outbreak the same vaccine was found not to offer absolute protection from infection, but infected people were found to suffer fewer symptoms, recovered more quickly, and were less likely to die. Vaccinated people were found to be producing antibodies to the Virus six months after they were vaccinated. It is unclear whether natural immunity, or the immunity offered by vaccination, wanes over time for Ebolavirus.
See also...










%20(1)%20(1).png)







%20(1)%20(1).png)











-by-date-of-symptom-onset-in-the-united-republic-of-tanzania--as-of-31-may-2023.png)